
The elbow joint has become the focus of interest in recent years. Diverse disease patterns in childhood and adulthood lead to problems with the elbow joint. On the one hand, free joint bodies can acutely block the movement in the elbow joint, inserting tendons can be degenerative and even tear, post-traumatic malpositions or soft tissue contractures lead to massive movement restrictions. Both open and arthroscopic, reconstructive and endoprosthetic procedures are recognized surgical techniques. In the following, the most common symptoms of the elbow and suitable therapy options are presented to you.
- Tennis elbow (Epicondylopathia humeri radialis)
- Free joint bodies, osteochondrosis dissecans
- Stiff elbow
- Rupture of the distal biceps and triceps tendons
- Elbow instabilities
- Fractures of the elbow joint
- Osteoarthritis of the elbow joint
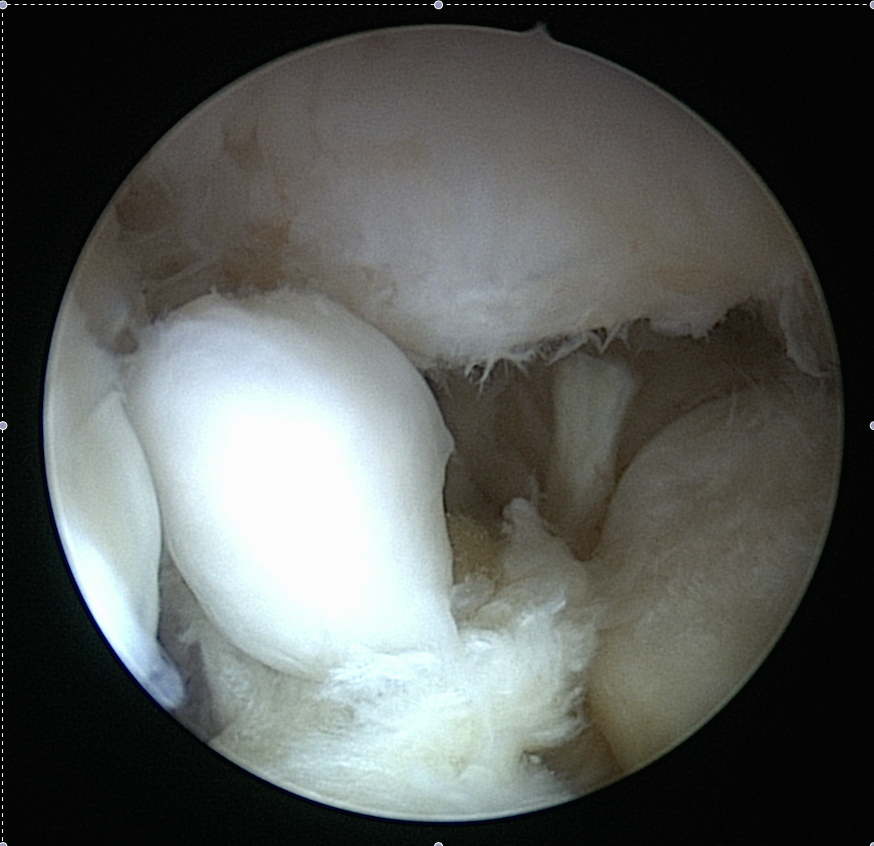
Free joint body in the elbow joint in the intraoperative findings
Tennis elbow
The epicondylopathia humeri radialis, also known colloquially as tennis elbow, is caused by overuse in the area of the extensor tendons with an attachment to the outer protruding bone of the elbow joint. The focus is primarily on conservative therapy with physiotherapy and, if necessary, infiltration therapy. If the symptoms persist, any surgical therapy should be reconsidered, which can be carried out minimally invasively (arthroscopically) or openly.
Free joint bodies, osteochondrosis dissecans
For reasons that are not yet fully understood, bone tissue may break down in young, often sporty patients. As the disease progresses, the under-supplied bone separates and, as a free joint body in the elbow joint, leads to complaints and blockages in movement. Here, too, there is stage-appropriate therapy in the form of arthroscopic or open procedures. Free joint bodies can also occur in the course of degenerative processes, which can easily be removed using elbow joint arthroscopy (see illustration).
Stiff elbow
An elbow joint stiffness can occur as a consequence of an accident or as part of degenerative processes. This is treated by elbow arthroscopy by removing excess bone and removing the thickened capsule. In the case of large ossifications (heterotopic ossifications), however, the joint sometimes has to be opened and the protruding bones removed. After the operation, further treatment takes place on a motorized splint in order to maintain the mobility that has been gained.
Rupture of the biceps and triceps tendons at the elbow joint
Heavy physical activity as well as incorrect sporting activities can lead to tearing of the large flexor (biceps) or extensor tendon (triceps tendon) at the elbow joint. In the case of non-surgical treatment, a loss of strength can occur, so that reattachment (refixation) of the tendon is usually recommended surgically. This is usually achieved by inserting anchors into the bone. It takes about 12 weeks to heal.
Elbow instabilities
A traumatic dislocation of the elbow joint (elbow dislocation) can in some cases result in an operation in which the stabilizing collateral ligaments are sutured again. If dislocations occur again and again, the only option is to replace them with a ligament replacement with the help of another tendon from the elbow joint, knee joint or the tissue bank. Postoperatively, the immobilization takes place in a splint, which allows an axially correct movement without stressing the newly reconstructed ligaments. Here, too, a minimum healing period of around 12 weeks can be expected.
Fractures of the elbow joint
The elbow joint consists of the humerus and two forearm bones, which are connected by two joint compartments. In addition to the extension and flexion, the elbow joint is also involved in the turning movement. A direct impact trauma on the elbow or a fall on the outstretched arm can lead to fractures with and without dislocation of the joint, some of which require an operation. Screws and plates are inserted to stabilize the fracture. In some cases, the reconstruction of the articular surface is not possible, so that, for example, the spoke head has to be replaced by a radius head prosthesis.
Osteoarthritis of the elbow joint
Post-traumatic secondary conditions or various forms of osteoarthritis can lead to a complete destruction of the joint, so that joint-preserving therapy is no longer possible. The implantation of an artificial elbow joint implies a reduction in the carrying weight of the affected extremity to 5kg. Because of this, the indication for implantation is only to be made if there is a strict indication.
Current research projects
In the area of elbow pathologies, there are still many unanswered questions, so that research at the Center for Musculoskeletal Surgery is also concerned with clarifying these questions. The main focus is on elbow instability, possible forms of cell therapy for cartilage damage to the elbow joint and alternative forms of therapy for the treatment of the tennis elbow joint.